

What Is Treatment-Emergent Central Apnea?
Treatment-emergent central apnea (TECA), also called complex sleep apnea syndrome, is a pattern where central apneas appear — or significantly increase — after starting CPAP therapy. It's distinct from obstructive sleep apnea: in central apnea, your airway is open but your brain briefly stops sending the signal to breathe.
The American Academy of Sleep Medicine (AASM) defines TECA as the emergence of a central apnea index (CAI) of ≥ 5 per hour during CPAP titration or treatment, in someone who originally had predominantly obstructive events.
TECA is more common than most people realize. Studies estimate it appears in 5–15% of patients starting CPAP therapy. For most, it resolves on its own within 1–3 months as the brain's respiratory control adapts.
Why Does It Happen?
The mechanism isn't fully understood, but the leading explanation involves CO₂ and respiratory drive:
Your brainstem uses CO₂ levels to regulate breathing. CPAP-delivered pressure "washes out" CO₂ — particularly with higher pressures and expiratory pressure relief (EPR) — and when CO₂ drops below the apnea threshold, the brain's drive to breathe momentarily pauses.
CPAP also eliminates the arousal-inducing effort of fighting an obstructed airway. When that stimulus is removed, some patients' respiratory control systems — which may have been relying on arousal as a backup cue — can become temporarily unstable.
Risk factors for TECA include:
- Higher CPAP pressure settings
- EPR set to high (2–3) on Full Time mode
- Pre-existing Cheyne-Stokes breathing or heart failure
- Opioid or sedative use
- Older age
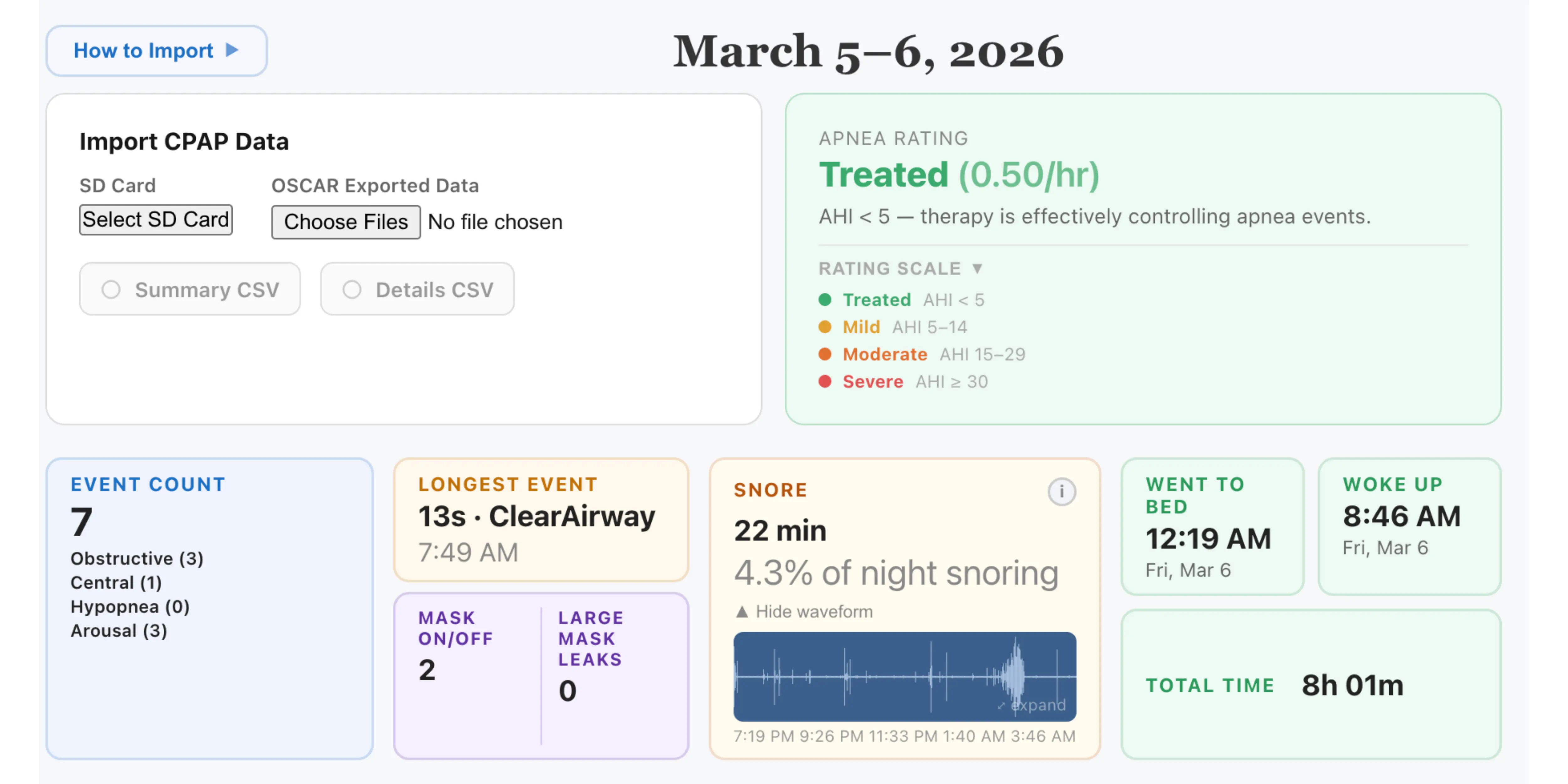
What Your Data Shows
On your CPAP data, TECA looks like a high central apnea index alongside a low or normal obstructive apnea index — the opposite of what you'd expect from straightforward OSA.
Signs to look for in CPAP Insights:
- Central apnea proportion: if CA events make up more than 50% of your total apnea events, TECA is worth discussing with your doctor
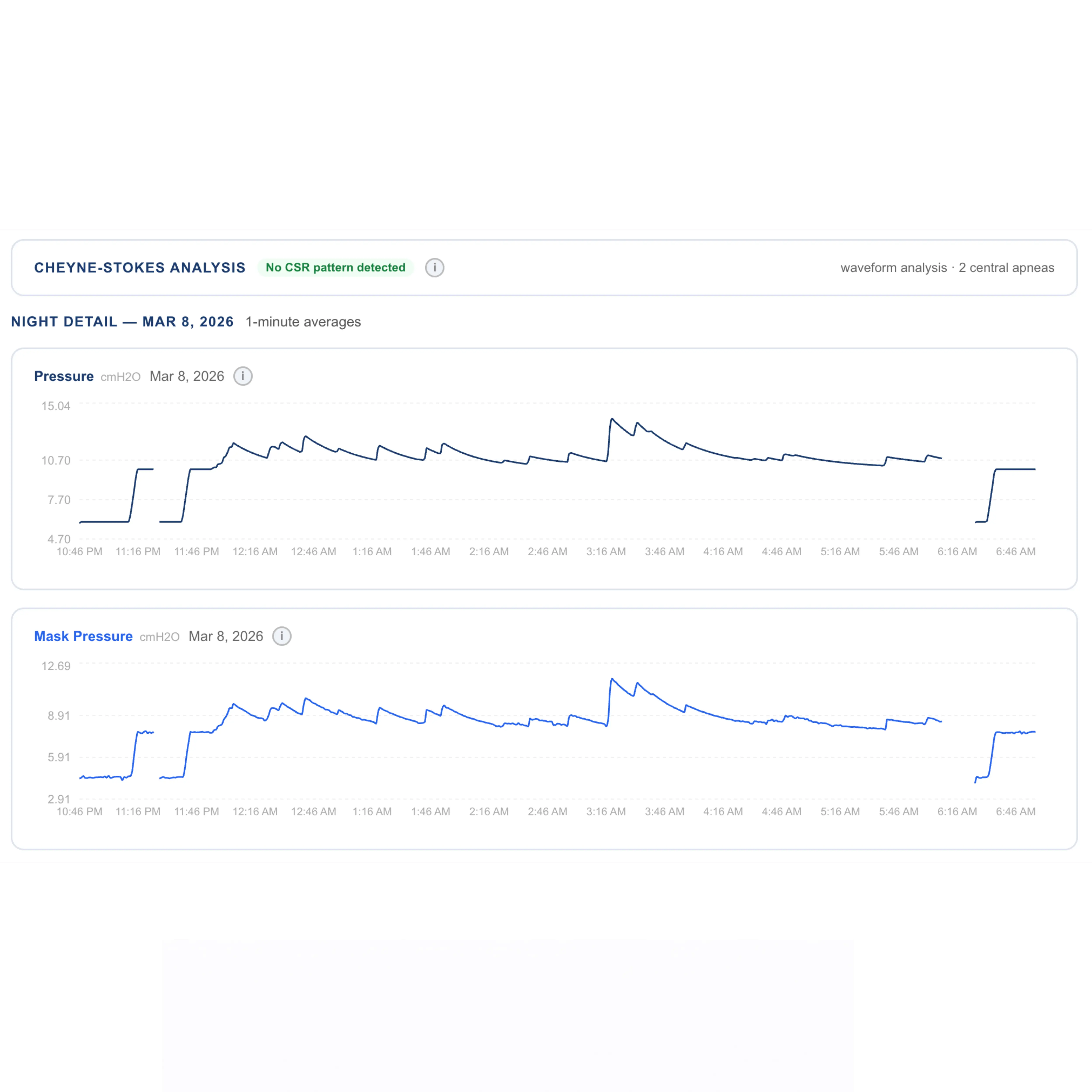
- Periodic clustering: central events often appear in groups with a cyclical breathing pattern (crescendo-decrescendo Tidal Volume) — the Cheyne-Stokes signature
- Pressure correlation: central events may cluster when the machine is at higher pressure or when EPR is active
- Time-of-night pattern: TECA events often predominate in lighter sleep stages (N1/N2) in the second half of the night
CPAP Insights calculates your central apnea index, total CA count, and CA proportion to help you identify these patterns before your next appointment.
Does It Resolve on Its Own?
For the majority of TECA cases, yes. Multiple studies show that central apneas diminish significantly within 8–12 weeks as the respiratory control system adapts to consistent CPAP pressure. Follow-up data often shows a return to predominantly obstructive — or near-zero — event profiles without any intervention.
Monitoring your data over time is the most useful thing you can do. If your CA index is elevated in the first 2–4 weeks but trending down week over week, that's a reassuring pattern. If it's stable or increasing after 6–8 weeks, bring the data to your sleep doctor.
When to Talk to Your Sleep Doctor
Consult your sleep doctor if:
- Your central apnea index exceeds 5/hr and CA events are more than 50% of all events
- You're not seeing improvement after 6–8 weeks of consistent therapy
- You have known heart failure, atrial fibrillation, or neurological conditions that can cause central events
- You feel your therapy is ineffective despite good compliance and a low obstructive AHI
Treatment options for persistent TECA include reducing EPR to minimum or Off, lowering maximum pressure, or switching to Adaptive Servo-Ventilation (ASV) — a mode specifically designed to stabilize respiratory drive. These decisions should be made with your sleep specialist based on a full clinical picture, not self-adjustment.